

 Previous
Previous
Challenging cases
Case 1 - The case of the indecipherable orders

Writing orders, reading orders, transcribing orders ... written communication is a central part of in-hospital care. It is also the place where medication errors can begin and a high-yield area for patient safety intervention!
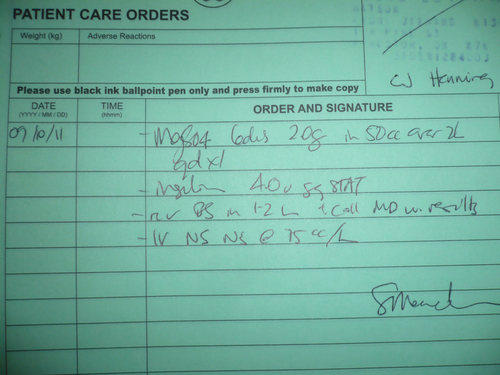
Answer the questions below based on the orders provided.
Potentially Dangerous Abbreviations[2]
DO NOT USE | USE INSTEAD |
U, u (unit) | Write "unit" |
IU (International Unit) | Write "International Unit" |
Q.D., QD, q.d., qd, O.D.,OD (daily) | Write "daily" |
Q.O.D., QOD, q.o.d., qod, E.O.D., EOD, e.o.d., eod, (every other day) | Write "every other day" |
Trailing zero (X.0 mg) | Write X mg |
Lack of leading zero (.X mg) | Write 0.X mg |
MS | Write morphine sulfate |
MSO4, MgSO4 | Write Magnesium sulfate |
AVOID USING | |
< (less than)> (greater than) | Write "less than"Write "greater than" |
Abbreviations for drug names | Write drug names in full |
@ | Write "at" |
cc | Write "mL" (preferred) or "ml" or "millilitres" |
"One of the major causes of medication errors is the ongoing use of potentially dangerous abbreviations and dose expressions. Underlying factors contributing to many of these errors are illegible or confusing handwriting by clinicians and the failure of health care providers to communicate clearly with one another."[2]
_________________________________
2. The Joint Commission. Sentinel Event Alert. Medication errors related to potentially dangerous abbreviations. Issue 23 - September 1, 2001. Available from: www.jointcommission.org/sentinelevents/sentineleventalert/sea_23.htm